Omicron Mutation
South African genomic scientists said earlier this week the variant has an unusually high number of mutations, with more than 30 in the key spike protein -- the structure the virus uses to get into the cells they attack.
To compare, the Delta variant has 13 mutations.
 www.sciencefocus.com
www.sciencefocus.com
Discovered Nov 9.
 www.who.int
www.who.int
The discovery of the omicron variant has coincided with a spike in South African cases — a 1,124 percent increase over the past two weeks.
It also has mutations that are known to increase the infectivity, fitness, and virulence of SARS-CoV-2.
 www.sciencedirect.com
www.sciencedirect.com
Another mutation, N501Y, appears to increase the ability of the virus to gain entry to our cells, making it more transmissible.
 www.independent.co.uk
www.independent.co.uk

How Did It Get Created? “B.1.1.529 is likely to have evolved during a chronic infection of an immuno-compromised person, possibly in an untreated HIV/AIDS patient.” This is believed to be the source of the Alpha variant, an immuno-compromised person patient in England. “In the United States, the Alpha variant first appeared late November 2020, grew from 1.2% in late January and became predominant around the end of March 2021.” It was then replaced by the Delta Variant. It was first detected in India in late 2020. The Delta variant was named on 31 May 2021 and had spread to over 163 countries by 24 August 2021. Note: It took six months for WHO to name the Delta Variant, it has named Omicron in three days!
The Reaction:
“Countries around the world moved to restrict travel from southern Africa on Friday in a frantic effort to keep a
newly identified, and apparently significantly evolved, variant of the coronavirus from crossing their borders.
The European Commission proposed that its members activate the “emergency brake” on travel from
countries in southern African and other countries affected to limit the spread of the new variant.
“All air travel to these countries should be suspended until we have a clear understanding about the danger
posed by this new variant,” Ursula von der Leyen, the president of the European Union’s executive arm, said
in a statement. “And travelers returning from this region should respect strict quarantine rules.”
“Late on Thursday Britain said it was suspending flights temporarily from South Africa, Botswana, Lesotho,
Eswatini, Namibia and Zimbabwe. When they start up again, British and Irish citizens returning from these
countries will be required to quarantine in government-approved hotel facilities.” “Any British residents arriving
from South Africa after Sunday morning must stay at a government approved
hotel for 11 nights at a cost of £2,285 per person.
“The Biden administration will restrict travel from South Africa and seven other African countries to try to contain the new variant of the coronavirus, senior administration officials said on Friday. Starting on Monday, the administration will prohibit travelers from South Africa, Botswana, Zimbabwe, Namibia, Lesotho, Eswatini, Mozambique and Malawi from coming to the United States, the officials said. The travel ban will not apply to American citizens or lawful permanent residents, officials said. But they will need to show a negative coronavirus test before coming to the United States.”
Summary of Medical Impact:
Attached are various news sources used above, with extractions highlighted. Below are some twitter references where other information was pulled from. Some quotes above pulled from webpages that are not included in PDFs:

 www.medrxiv.org
www.medrxiv.org
The researchers found that Omicron SARS-CoV-2 infects and multiplies 70 times faster than the Delta variant and original SARS-CoV-2 in human bronchus, which may explain why Omicron may transmit faster between humans than previous variants. Their study also showed that the Omicron infection in the lung is significantly lower than the original SARS-CoV-2, which may be an indicator of lower disease severity.
 www.med.hku.hk
www.med.hku.hk
South African genomic scientists said earlier this week the variant has an unusually high number of mutations, with more than 30 in the key spike protein -- the structure the virus uses to get into the cells they attack.
To compare, the Delta variant has 13 mutations.
Everything you need to know about the Delta variant of coronavirus
The variant is the dominant COVID strain in the UK. Here's what we know about Delta.
www.sciencefocus.com
Discovered Nov 9.
Classification of Omicron (B.1.1.529): SARS-CoV-2 Variant of Concern
The Technical Advisory Group on SARS-CoV-2 Virus Evolution (TAG-VE) is an independent group of experts that periodically monitors and evaluates the evolution of SARS-CoV-2 and assesses if specific mutations and combinations of mutations alter the behaviour of the virus. The TAG-VE was convened...
www.who.int
The discovery of the omicron variant has coincided with a spike in South African cases — a 1,124 percent increase over the past two weeks.
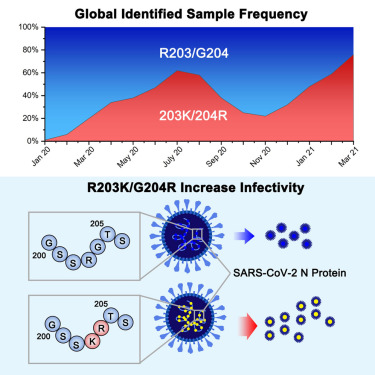
It also has mutations that are known to increase the infectivity, fitness, and virulence of SARS-CoV-2.
Nucleocapsid mutations R203K/G204R increase the infectivity, fitness, and virulence of SARS-CoV-2
Previous work found that the co-occurring mutations R203K/G204R on the SARS-CoV-2 nucleocapsid (N) protein are increasing in frequency among emerging …
www.sciencedirect.com
Another mutation, N501Y, appears to increase the ability of the virus to gain entry to our cells, making it more transmissible.
Everything we know about the new ‘omicron’ variant
B.1.1529 has ‘incredibly high’ number of mutations on its spike protein
www.independent.co.uk
Our vaccines are focused on identifying the virus based upon the genetic code of what is commonly called the “spike protein”. “SARS-CoV-2 is characterized by a spike protein allowing viral binding to the angiotensin-converting enzyme (ACE)-2, which acts as a viral receptor and is expressed on the surface of several pulmonary and extra-pulmonary cell types, including cardiac, renal, intestinal and endothelial cells.” The virus binds to the cell at the ACE-2 receptor site on the cell and then injects itself into the cell to replicate.
The strain is officially called B.1.1.529 and today the WHO designate the variant as the “Omicron variant”, using the Greek number classification system and labeled it a “variant of concern.” On the genomic epidemiology of novel coronavirus website, it is Clade 21K (see first attachment).
“Back in November 2020, when the alpha variant emerged, it was about 50 per cent more transmissible (as the Wuhan strain). This made a huge difference, and raised the herd immunity threshold from 66 per cent to almost 80 per cent. Today, with Delta, it is 85-90 per cent. The Delta variant, is more than twice as transmissible as the Wuhan strain.” “Data from South Africa’s National Institute for Communicable Diseases show how the new variant quickly crowded out the highly transmissible Delta variant over the past two weeks. It now makes up around 90% of infections in the country’s most populous province, home to its political and economic capitals of Pretoria and Johannesburg.” See the blue spike for November 2021 in the chart below.
Here are the two key issues that indicate this variant is a problem:
- “On the protein that helps to create an entry point for the coronavirus to infect human cells (i.e. just the receptor binding domain of the spike protein), the new variant has 10 mutations, many more than the dangerous Delta variant, Professor de Oliveira said.” (Another article said that the Delta variant had 2 changes on the receptor binding domain of the spike protein which is part of the reason for the need for the booster vaccinations. The changes in the Delta variant made is more difficult for our antibodies to easily identify the virus.) The new variant, B.1.1.529, has a “very unusual constellation of mutations,” with more than 30 in the spike protein alone, according to Tulio de Oliveira, director of the KwaZulu-Natal Research and Innovation Sequencing Platform. The new variant already accounts for 75% of the genomes tested in the country, De Oliveira said in a later tweet.” Note: “Some of the mutations have been detected in previous variants, such as Alpha and Delta, and have been associated with increased transmissibility and immune evasion. Many of the other identified mutations are not yet well characterized and have not been identified in other currently circulating variants.”
More specifically, here is a list of mutations and their potential impact:
- “South African scientists spotted a quirk in the testing regimen. PCR tests look for three genes in the coronavirus and amplify them. If, however, the virus was this variant they were only able to amplify two.” “This variant seems to give quirky results (known as an S-gene dropout, see also this) in the standard tests and that can be used to track the variant without doing a full genetic analysis. That suggests 90% of cases in Gauteng may already be this variant and it "may already be present in most provinces" in South Africa.”
How Did It Get Created? “B.1.1.529 is likely to have evolved during a chronic infection of an immuno-compromised person, possibly in an untreated HIV/AIDS patient.” This is believed to be the source of the Alpha variant, an immuno-compromised person patient in England. “In the United States, the Alpha variant first appeared late November 2020, grew from 1.2% in late January and became predominant around the end of March 2021.” It was then replaced by the Delta Variant. It was first detected in India in late 2020. The Delta variant was named on 31 May 2021 and had spread to over 163 countries by 24 August 2021. Note: It took six months for WHO to name the Delta Variant, it has named Omicron in three days!
The Reaction:
“Countries around the world moved to restrict travel from southern Africa on Friday in a frantic effort to keep a
newly identified, and apparently significantly evolved, variant of the coronavirus from crossing their borders.
The European Commission proposed that its members activate the “emergency brake” on travel from
countries in southern African and other countries affected to limit the spread of the new variant.
“All air travel to these countries should be suspended until we have a clear understanding about the danger
posed by this new variant,” Ursula von der Leyen, the president of the European Union’s executive arm, said
in a statement. “And travelers returning from this region should respect strict quarantine rules.”
“Late on Thursday Britain said it was suspending flights temporarily from South Africa, Botswana, Lesotho,
Eswatini, Namibia and Zimbabwe. When they start up again, British and Irish citizens returning from these
countries will be required to quarantine in government-approved hotel facilities.” “Any British residents arriving
from South Africa after Sunday morning must stay at a government approved
hotel for 11 nights at a cost of £2,285 per person.
“The Biden administration will restrict travel from South Africa and seven other African countries to try to contain the new variant of the coronavirus, senior administration officials said on Friday. Starting on Monday, the administration will prohibit travelers from South Africa, Botswana, Zimbabwe, Namibia, Lesotho, Eswatini, Mozambique and Malawi from coming to the United States, the officials said. The travel ban will not apply to American citizens or lawful permanent residents, officials said. But they will need to show a negative coronavirus test before coming to the United States.”
Summary of Medical Impact:
- Effectiveness of current vaccines will not be known for about two weeks based upon what I have read.
- “Antibody therapies, used for immunocompromised people, could be seriously undermined.
- “Antivirals, however, which attack the enzymes used by the virus, will be unaffected.”
Attached are various news sources used above, with extractions highlighted. Below are some twitter references where other information was pulled from. Some quotes above pulled from webpages that are not included in PDFs:
- https://twitter.com/Tuliodna Director of CERI: Centre for Epidemic Response & innovation, South Africa
- https://twitter.com/PeacockFlu/status/1463176821416075279 Virologist at @ImperialInfect; Viruses, Influenza, SARS-CoV-2 and Variants
- https://twitter.com/jburnmurdoch/status/1463956686075580421 Stories, stats & scatterplots for @FinancialTimes
Saliva swabs are the preferred sample for Omicron detection
The Omicron variant is characterised by more than 50 distinct mutations, the majority of which are located in the spike protein. The implications of these mutations for disease transmission, tissue tropism and diagnostic testing are still to be determined. We evaluated the relative performance...
www.medrxiv.org
The researchers found that Omicron SARS-CoV-2 infects and multiplies 70 times faster than the Delta variant and original SARS-CoV-2 in human bronchus, which may explain why Omicron may transmit faster between humans than previous variants. Their study also showed that the Omicron infection in the lung is significantly lower than the original SARS-CoV-2, which may be an indicator of lower disease severity.
HKUMed finds Omicron SARS-CoV-2 can infect faster and better than Delta in human bronchus but with less severe infection in lung
HKUMed provides the first information on how the novel Variant of Concern of SARS-CoV-2, the Omicron SARS-CoV-2, infect human respiratory tract.
www.med.hku.hk
Last edited:





")




